
Peptide Therapy for Inflammation and Recovery: What You Need to Know
Share this Post
Chronic inflammation is at the root of many persistent pain conditions, from tendinitis and arthritis to post-surgical complications and autoimmune disorders. Traditional treatments like NSAIDs and corticosteroids provide temporary relief but come with significant drawbacks.
Peptide therapy for inflammation offers a fundamentally different approach. Rather than simply suppressing symptoms, therapeutic peptides work at the cellular level to modulate inflammatory pathways while simultaneously promoting tissue repair. As a board-certified pain management physician specializing in regenerative medicine, I have witnessed how peptide therapy can transform outcomes for patients struggling with chronic inflammation and slow-healing injuries.
What Are Therapeutic Peptides?
Peptides are short chains of amino acids, typically containing between 2 and 50 building blocks, that function as signaling molecules throughout your body. Your body naturally produces thousands of different peptides that coordinate inflammation resolution, wound healing, and tissue maintenance.
Therapeutic peptides either replicate these natural signals or enhance their activity. Unlike small-molecule drugs that often have broad, systemic effects, peptides are large enough to target specific biological pathways yet small enough to penetrate tissues and reach injured areas effectively.
The medical use of peptides dates back to the 1920s with the isolation of insulin, which transformed diabetes care. Today, peptide therapy has evolved into a sophisticated field, with FDA-approved medications like semaglutide demonstrating the therapeutic potential of this approach. In regenerative medicine, peptides like BPC-157, TB-500, and GHK-Cu are gaining recognition for their ability to reduce inflammation and accelerate healing.
How Peptides Reduce Inflammation
Understanding how peptide therapy for inflammation works requires looking at the biological pathways involved. Unlike NSAIDs that block a single enzyme, therapeutic peptides target multiple interconnected mechanisms.
Cytokine Modulation
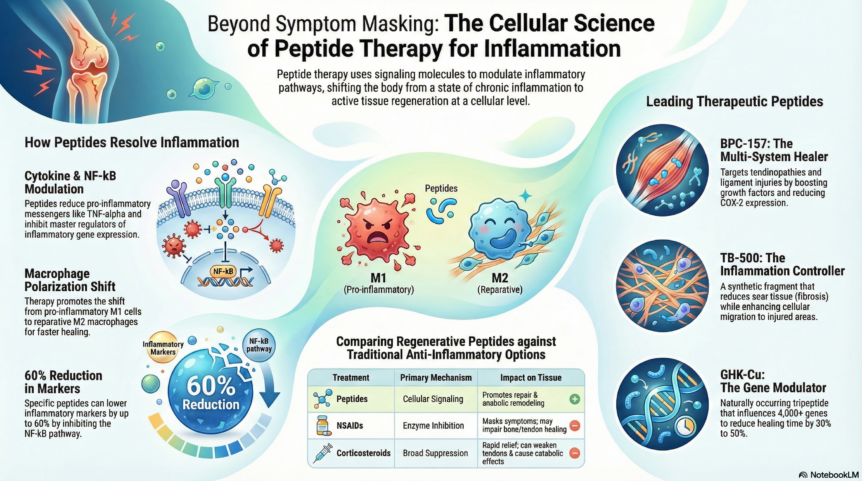
Pro-inflammatory cytokines like TNF-alpha, IL-6, and IL-1beta drive the inflammatory cascade that causes pain, swelling, and tissue damage. Therapeutic peptides significantly reduce production of these inflammatory messengers while promoting anti-inflammatory signals. This creates a shift from chronic inflammation toward resolution and healing.
NF-kB Pathway Inhibition
Nuclear factor-kappa B is a master regulator of inflammatory gene expression. When activated, it triggers production of inflammatory proteins throughout the body. Peptides like GHK-Cu and KPV inhibit NF-kB activation, reducing inflammatory markers by up to 60 percent in some studies. This represents a more targeted approach than corticosteroids, which broadly suppress immune function.
Macrophage Polarization
Your immune system contains macrophages that can either promote inflammation (M1 type) or support tissue repair (M2 type). Chronic inflammation often involves an overabundance of M1 macrophages. BPC-157 promotes the shift from pro-inflammatory M1 to reparative M2 macrophages, facilitating inflammation resolution and reducing scar tissue formation.
Antioxidant Enhancement
Oxidative stress amplifies inflammation and damages tissues. GHK-Cu enhances superoxide dismutase activity and upregulates protective enzymes, bolstering your body’s antioxidant defenses. This protects cells from oxidative damage while reducing the inflammatory burden.
Key Peptides for Inflammation and Recovery
Several peptides have emerged as particularly effective for reducing inflammation and promoting tissue repair.
BPC-157: The Multi-System Healer
Body Protection Compound-157 is derived from a protective protein found in human gastric juice. This 15-amino-acid peptide demonstrates remarkable stability and can be administered orally or by injection.
BPC-157 reduces pro-inflammatory cytokines including IL-6, TNF-alpha, and interferon-gamma while decreasing COX-2 gene expression. A 2025 systematic review in orthopedic sports medicine concluded that BPC-157 promotes healing by boosting growth factors and reducing inflammation, with improved structural and functional recovery across fracture, muscle, tendon, and ligament injury models.
Clinical observations report that patients using BPC-157 experience significant improvements in mobility and pain reduction, with some noting relief lasting six months or longer. The peptide works particularly well for tendinopathies, ligament injuries, muscle strains, and gastrointestinal inflammation.
TB-500: The Inflammation Controller
TB-500 is a synthetic fragment of thymosin beta-4, a peptide naturally produced by the thymus gland. Its anti-inflammatory mechanisms include reducing TNF-alpha production, downregulating NF-kB activation, and decreasing oxidative stress through enhanced antioxidant enzyme activity.
A distinguishing feature of TB-500 is its anti-fibrotic activity. By promoting organized collagen deposition and reducing myofibroblast activity, TB-500 minimizes scar tissue formation. In animal models of muscle injury, TB-500-treated tissues demonstrate less fibrosis, better vascularization, and superior biomechanical properties compared to untreated controls.
TB-500 finds primary use in soft tissue injuries, chronic tendinopathies, joint inflammation, and post-surgical recovery. Its longer half-life allows for less frequent dosing, typically twice weekly.
GHK-Cu: The Gene Modulator
Glycyl-L-histidyl-L-lysine-copper is a naturally occurring tripeptide that influences over 4,000 genes involved in tissue repair and inflammation resolution. First identified in human plasma in the 1970s, GHK-Cu demonstrates remarkable biological versatility.
Studies demonstrate that GHK-Cu reduces inflammatory markers in tissue by up to 60 percent, significantly lowering levels of TNF-alpha, IL-6, and other pro-inflammatory cytokines. The peptide also stimulates collagen and elastin production, enhances fibroblast activity, and promotes organized tissue remodeling.
In wound healing, GHK-Cu reduces healing time by 30 to 50 percent across surgical wounds, chronic ulcers, and traumatic injuries. Its anti-inflammatory and antioxidant properties make it valuable for conditions where oxidative stress impairs recovery.
KPV: The Intracellular Anti-Inflammatory
KPV is a tripeptide derived from alpha-melanocyte-stimulating hormone. What distinguishes KPV from other anti-inflammatory agents is its ability to work inside cells rather than on cell surface receptors.
KPV enters cells via a transporter that is upregulated in inflamed tissues, providing targeted delivery to areas of active inflammation. Once inside, it inhibits NF-kB and MAPK cascades, preventing production of pro-inflammatory cytokines at the transcriptional level.
KPV is particularly valuable for inflammatory bowel diseases, autoimmune conditions, and chronic systemic inflammation. Its targeted mechanism allows for potent anti-inflammatory effects without broad immune suppression.
Thymosin Alpha-1: The Immune Balancer
Thymosin alpha-1 is a 28-amino-acid peptide that modulates both innate and adaptive immunity. What makes it unique is its dual capacity: enhancing immunity when needed while dampening excessive inflammation.
The peptide reduces pro-inflammatory cytokines including TNF-alpha, IL-1beta, and IL-6, and inhibits M1 macrophage activation. A 2025 meta-analysis found that Thymosin Alpha-1 significantly reduced the incidence of secondary infections in patients with severe inflammatory conditions.
For pain management, Thymosin Alpha-1 proves valuable in autoimmune-driven inflammation, chronic fatigue syndromes, and conditions where immune dysregulation contributes to tissue damage.
Conditions That Respond to Anti-Inflammatory Peptide Therapy
Peptide therapy for inflammation shows promise across a diverse range of conditions.
Acute Sports Injuries: Tendon and ligament sprains, muscle tears, and overuse injuries respond well to peptide therapy. Peptides offer alternatives to prolonged rest, NSAIDs, or premature corticosteroid injections that can weaken tissues.
Chronic Tendinopathies: Conditions like tennis elbow, Achilles tendinopathy, and rotator cuff tendinitis that have not responded to conservative management may benefit from peptides. These compounds address underlying pathology including collagen disorganization, persistent inflammation, and impaired blood supply.
Post-Surgical Recovery: Peptides can accelerate tissue integration, reduce post-operative inflammation, and minimize scar tissue formation following joint replacements, ligament reconstructions, or soft tissue repairs.
Osteoarthritis: By promoting cartilage metabolism and reducing inflammatory cytokines, peptides offer a regenerative alternative to repeated corticosteroid injections that can accelerate cartilage degradation.
Autoimmune-Mediated Pain: Conditions like rheumatoid arthritis where immune dysregulation drives inflammation and tissue damage may respond to immune-modulating peptides like Thymosin Alpha-1 and KPV.
Gut-Related Inflammation: For patients where gastrointestinal pathology drives systemic inflammation, BPC-157 and KPV target gut healing and inflammatory resolution. Many systemic inflammatory conditions have gastrointestinal components that benefit from this approach.
The Power of Combination Protocols
Research on peptide combinations demonstrates synergistic effects that exceed the sum of individual components. A 2021 study on regenerative peptides found that combinations exhibited synergistic changes in gene expression compared to individual peptides alone.
Combination protocols leverage three principles. First, complementary actions where peptides target different aspects of the same process. BPC-157 accelerates tissue repair while TB-500 reduces inflammation and enhances cellular migration, creating optimal conditions for healing. Second, sequential enhancement where one peptide creates conditions that enhance the effectiveness of others. Third, multi-pathway activation that addresses both upstream and downstream targets in the healing cascade.
Studies comparing combination protocols to single-peptide therapy show consistently superior outcomes: faster healing with 30 to 50 percent reduction in recovery time, more complete tissue regeneration, reduced inflammation, and improved patient-reported outcomes.
Common combinations include BPC-157 plus TB-500 plus GHK-Cu for soft tissue injuries, and KPV plus BPC-157 for gut-mediated systemic inflammation. The specific protocol depends on the condition being treated and individual patient factors.
How Peptides Compare to Traditional Anti-Inflammatory Treatments
Peptides vs. NSAIDs
NSAIDs inhibit cyclooxygenase enzymes, reducing prostaglandin synthesis and thereby inflammation and pain. While effective for symptom control, NSAIDs carry risks of gastrointestinal ulceration and bleeding, cardiovascular events, renal impairment, and impaired bone and tendon healing.
Peptides target inflammatory pathways while simultaneously promoting tissue repair. Unlike NSAIDs that mask symptoms by blocking prostaglandin synthesis, peptides modulate inflammation at the transcriptional level and enhance healing cascades. Importantly, peptides do not inhibit the inflammatory phase of healing that is necessary for cellular recruitment and debris clearance.
Peptides vs. Corticosteroids
Corticosteroids provide rapid symptom relief but carry substantial risks: immunosuppression, impaired wound healing, tendon weakening with increased rupture risk, hyperglycemia, and osteoporosis with chronic use.
Peptides offer anti-inflammatory effects without global immunosuppression or catabolic tissue effects. BPC-157, TB-500, and GHK-Cu reduce inflammatory cytokines while promoting anabolic tissue remodeling, which is the opposite of corticosteroid effects. For tendinopathies, this distinction is critical since corticosteroids can weaken already compromised tendons.
Peptides vs. Opioids
Opioids mask pain through central nervous system effects but carry risks of tolerance, dependence, overdose, and paradoxical opioid-induced hyperalgesia. They do nothing to address the underlying cause of pain.
Peptides modulate pain indirectly through inflammation reduction, tissue repair, and nerve regeneration. While not appropriate for acute severe pain requiring immediate analgesia, peptides may reduce chronic pain by addressing underlying pathology that perpetuates pain signaling. This represents an opportunity to reduce opioid prescribing and facilitate tapering in appropriate patients.
Safety Profile and What to Expect
Therapeutic peptides demonstrate favorable safety profiles across preclinical and observational human data. Most peptides are naturally occurring or derivatives of compounds your body already produces, which reduces immunogenicity and toxicity risks.
Common side effects, when they occur, are typically mild and transient. These may include injection site reactions such as redness, swelling, or tenderness that resolve within 24 to 48 hours. Some patients experience mild gastrointestinal symptoms, particularly with oral peptides, or transient fatigue during the adjustment period.
Improvements often begin within one to two weeks, with inflammation reduction and pain relief as early indicators of response. Maximal effects typically occur at four to six weeks, with full tissue remodeling continuing over three to six months.
Treatment cycles generally span four to eight weeks, depending on the condition. Some patients benefit from maintenance protocols for chronic conditions. Periodic treatment breaks are commonly recommended to prevent receptor adaptation and ensure continued responsiveness.
Is Peptide Therapy Right for Your Inflammatory Condition?
Peptide therapy for inflammation represents a paradigm shift in how we approach chronic pain and tissue damage. Rather than simply suppressing symptoms, we can now target the underlying inflammatory pathways while simultaneously promoting repair and regeneration.
At Core Medical & Wellness, we integrate peptide therapy as part of comprehensive, multimodal treatment plans. Peptides function optimally as adjuncts to physical therapy, nutrition optimization, and other regenerative approaches rather than isolated interventions.
Ideal candidates include patients with acute sports injuries seeking accelerated recovery, chronic tendinopathies that have not responded to conservative management, post-surgical orthopedic cases where optimized healing is a priority, inflammatory joint conditions where traditional treatments have fallen short, and autoimmune-mediated pain where immune modulation may provide benefit.
Whether peptide therapy is appropriate for your specific condition depends on a thorough evaluation of your symptoms, prior treatments, imaging findings, and overall health status. We encourage you to schedule a consultation to discuss whether peptide therapy might be a beneficial addition to your personalized treatment plan.
Medical Disclaimer: This article is for educational purposes only and should not be construed as medical advice. Most regenerative peptides are not FDA-approved and are available through compounding pharmacies. Peptide therapy recommendations must be made on an individual basis after appropriate clinical evaluation. Always consult with a qualified healthcare provider before beginning any new treatment. Results vary by individual.