

Menopause and Joint Pain: How HRT and New FDA Changes Can Help
Share this Post
If you are in your 40s or 50s and your knees, hands, or back suddenly ache more than they used to, you are not imagining things. More than half of women going through perimenopause and menopause report new or worse joint and muscle pain. And most of them are surprised to learn that hormones—not just aging—are a big part of the reason.
Below we break down why menopause makes joints hurt, how hormone replacement therapy (HRT) can fit into a pain-management plan, and what the recent FDA label changes mean for women thinking about treatment.
Why Do Joints Hurt During Menopause?
You may notice stiff fingers first thing in the morning, sore knees on the stairs, or an achy lower back that was never a problem before. These complaints are extremely common around the time periods slow down or stop. The timing is an important clue: shifting hormone levels—especially a drop in estrogen—play a direct role in how your joints feel.
Common patterns include:
- Hands and fingers — morning stiffness, weaker grip, and aching that eases slowly as you move.
- Knees and hips — pain going up or down stairs, getting out of a chair, or after sitting too long.
- Neck, shoulders, and back — tight, sore muscles that flare up with stress or poor sleep.
Sometimes imaging shows arthritis. Other times, X-rays look fine but the pain is very real. Doctors call this arthralgia—joint pain without visible inflammation. Either way, the drop in estrogen is often the trigger that turns a quiet problem into a daily one.
How Estrogen Protects Your Joints
Estrogen is much more than a reproductive hormone. Your cartilage, bones, muscles, and even your nervous system all have estrogen receptors. When estrogen levels fall at menopause, several things happen at once:
- Cartilage repair slows down and joints lose some of their natural cushioning and lubrication.
- Bone density drops, raising the risk of osteoporosis and stress fractures.
- Inflammation increases around the joints because estrogen’s calming effect on the immune system fades.
- Muscle mass decreases while body fat increases, putting more mechanical stress on the hips, knees, and spine.
- Pain sensitivity goes up because estrogen also helps regulate how your nervous system processes pain signals.
When you combine joint changes, muscle loss, poor sleep from hot flashes, and shifting mood and energy, you get the perfect setup for chronic pain. Old injuries or mild arthritis that never really bothered you can suddenly become a daily problem once estrogen drops.
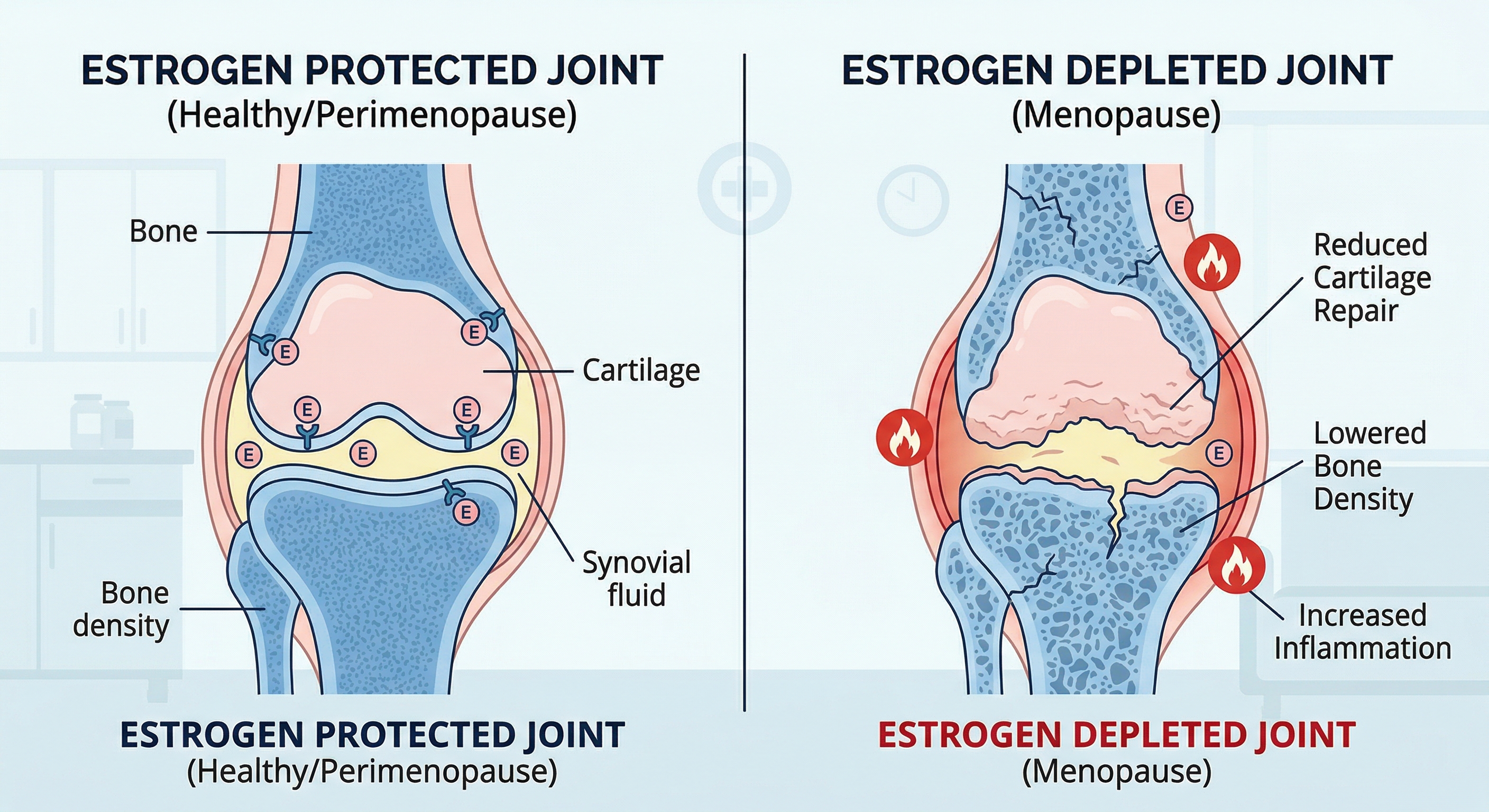
When estrogen levels drop during menopause, joints lose protective cushioning, bone density decreases, and inflammation rises — all of which contribute to pain and stiffness.
Can Hormone Replacement Therapy Help Joint Pain?
Hormone replacement therapy—also called menopausal hormone therapy—means giving back some of the estrogen (and often progesterone) your body has stopped making. HRT is mainly prescribed for moderate to severe hot flashes, night sweats, and other bothersome menopause symptoms. But many women and their doctors also notice improvements in joint and muscle pain.
Ways HRT May Support Your Joints
- Lowers inflammation in and around the joints.
- Helps maintain bone density and slows bone loss.
- Supports muscle mass and strength, especially when paired with exercise.
- Improves sleep and mood, which reduces overall pain sensitivity.
Some studies show that women using estrogen therapy report less knee pain and may be less likely to need a repeat surgery after joint replacement. Data from the Women’s Health Initiative found that estrogen-only therapy was linked to lower rates of hip replacement surgery.
For many women the benefit is partly indirect: when hot flashes cool down, sleep gets better, mood stabilizes, and there is more energy to exercise and rehabilitate the joints. Even small gains in those areas can add up to noticeably less daily pain.
What the Research Says Overall
Large reviews that combine many studies have found that HRT does not consistently reduce general body pain in every woman. Some research shows clear benefits for certain joint conditions; other studies show little difference.
In plain terms: HRT is not a dedicated joint-pain drug, and it will not erase structural arthritis. But for the right person at the right time, optimizing hormones can be a meaningful piece of the pain-management puzzle.
The 2025–2026 FDA Label Changes: What You Need to Know
For over 20 years, many women were told to stay away from hormone therapy because of fears raised by the Women’s Health Initiative (WHI) study in the early 2000s. That study led to strict “black box” warnings on HRT products, and the number of women using hormones dropped dramatically.
Since then, researchers have looked at the data much more carefully. They found that when healthy women start HRT before age 60 or within about 10 years of their last period, the risk-benefit picture looks very different from what the original headlines suggested.
In November 2025, the FDA announced it would begin removing the broad black box warnings from HRT products. By February 2026, the first six hormone therapy products received updated labels. Here is what changed:
- Warnings about heart disease, breast cancer, and dementia were removed from the boxed-warning section of six HRT products across all four therapy categories.
- The endometrial cancer warning stays for systemic estrogen-only products used by women who still have a uterus.
- Labels now highlight both benefits and risks more accurately, noting that women who start HRT within 10 years of menopause may see lower rates of death from all causes and fewer fractures.
- Twenty-nine drug companies have submitted updated labels, and more approvals are expected.
Why This Matters for Joint Pain
If you are a woman in your 40s or 50s dealing with new joint pain plus hot flashes, poor sleep, and low energy, you no longer have to assume HRT is off the table because of outdated fears. The updated guidance gives you and your doctor more room to talk honestly about:
- Your personal risk factors (family history of breast cancer, stroke, or blood clots).
- How severe your symptoms are and how much they affect daily life.
- Whether adding hormone therapy might improve your ability to stay active, protect your bones, and manage joint pain—on top of relieving hot flashes.
Who Should Consider HRT for Joint Pain?
Generally, women who may be good candidates to discuss HRT with their doctor include those who:
- Are younger than 60 and within about 10 years of their last period.
- Have moderate to severe hot flashes, night sweats, or sleep problems.
- Have new or worsening joint or muscle pain that is hurting their quality of life.
- Do not have a history of estrogen-sensitive cancer, stroke, serious blood clots, or other major reasons to avoid hormones.
If you fit that profile, HRT may offer several benefits at once: symptom relief, better sleep, bone protection, and possibly more comfortable joints—especially when combined with exercise, healthy eating, and targeted pain treatments.
Women who have had breast cancer, blood clots, stroke, or certain other conditions usually need a different path. Many non-hormonal options can still help a great deal.
How a Pain and Regenerative Medicine Specialist Can Help
Menopause-related joint pain sits at the crossroads of hormones, body mechanics, inflammation, and the nervous system. A pain and regenerative medicine specialist approaches the problem from multiple angles:
Step 1 — Thorough Evaluation
A careful workup helps tell the difference between menopause-related pain, osteoarthritis, tendon problems, and autoimmune conditions. This usually includes a detailed history of your symptoms, menstrual changes, sleep, and mood; a physical exam; imaging such as X-ray, ultrasound, or MRI when needed; and lab work to check for inflammation, metabolic health, and bone health.
Step 2 — A Layered Treatment Plan
Hormone therapy—if appropriate—is just one layer. A strong plan often includes:
- Targeted exercise and strength training to rebuild muscle, take stress off joints, and improve mobility.
- Weight management and nutrition support to ease pressure on the knees, hips, and spine.
- Medications when needed, such as short-term anti-inflammatories or other pain-relief options matched to your health profile.
- Regenerative treatments like platelet-rich plasma (PRP) when indicated, to support healing in damaged joints, tendons, or ligaments.
- Sleep and stress strategies, because poor sleep and chronic stress turn up the body’s pain volume.
If you are a good candidate for HRT, your pain specialist can work with your gynecologist or menopause provider to make sure your hormone plan and your pain plan support each other.
Questions to Bring to Your Doctor
If you are thinking about hormone therapy for menopause-related joint pain, consider asking:
- Could menopause be contributing to my joint and muscle pain?
- Based on my age and health history, am I a candidate for HRT?
- What benefits can I realistically expect for joint pain, sleep, and daily function?
- What are the main risks for someone like me, and how will we monitor them?
- If HRT is not right for me, what other options can help with both pain and menopause symptoms?
The right plan is always personalized. For some women, HRT becomes a cornerstone of symptom control and long-term bone and joint health. For others, non-hormonal approaches are safer and work just as well. The key is that you now have better information—and more supportive guidelines—to make an informed choice.
Bottom Line
Menopause-related joint pain is real, it is common, and it is not just “getting old.” Falling estrogen affects your cartilage, bones, muscles, and pain pathways all at once. Hormone replacement therapy is not a magic fix for arthritis, but for the right woman at the right time, it can be a powerful part of a bigger plan that includes exercise, weight management, and targeted pain treatments.
Thanks to the 2025–2026 FDA label updates, the conversation around HRT is finally catching up with the science. If you are struggling with joint pain, hot flashes, poor sleep, or all three, talk to your doctor about whether hormone therapy belongs in your treatment plan.
This article is for educational purposes only and does not replace medical advice. Always consult your healthcare provider before starting or changing any treatment.